1 Section of Neurosurgery, Department of Surgery, University of Manitoba. 2 Assistant Professor of Neurosurgery, Section of Neurosurgery, Department of Surgery, Rady Faculty of Health Sciences, University of Manitoba.
Abstract: Cauda equina syndrome (CES) is the collection of signs and symptoms produced by severe compression of the lumbar spinal nerves that form the cauda equina. The compression can be caused by lumbar degenerative changes, intraspinal tumors, epidural hematoma, and infections. Rapid diagnosis and treatment are paramount as CES requires emergent surgical decompression. With delay, the patient could develop permanent neurological deficits including loss of lower limb sensorimotor function, bladder, bowel, and/or sexual dysfunction. Unfortunately, even with expeditious surgery, neurological improvements remain unpredictable. Failure to fully explain the possible prognoses can involve all the healthcare providers in medicolegal consequences.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
1. Cauda Equina Syndrome results from pathologies that compress the nerves in the lumbosacral spinal canal, most commonly due to an acute lumbar disc herniation.
2. Early diagnosis is crucial and is made clinically by distinctive symptoms of saddle anesthesia, acute urinary incontinence combined with acute back and leg pain.
3. The most consistent early clinical sign of CES is urinary retention, and the prognosis is worse when present.
4. Urgent MRI is the study of choice and should be performed to confirm or rule out CES.
5. Surgery is highly recommended within 24 hours after CES is identified.
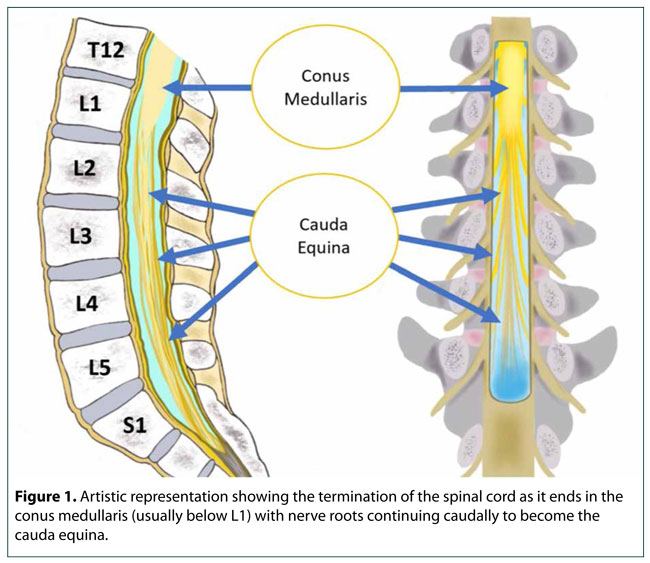
1. Cauda Equina Syndrome is caused by a large space-occupying lesion within the central canal of the lumbosacral spine, most commonly a large disc herniation. However, compression can also be caused by lumbar degenerative changes, intraspinal tumors, epidural hematoma, and infections.
2. Cauda equina syndrome generally presents with varying degrees of sensory loss and motor weakness in the lower extremities, saddle anesthesia, and bowel/bladder dysfunction (these last 2 are required to establish the diagnosis of CES).
3. The main clinical feature between differentiating Cauda Equina Syndrome vs Conus Medullaris Syndrome, is the absence of UPPER MOTOR NEURONS findings in CES).
4. About 70% of patients with cauda equina syndrome have a previous history of lower back pain and/or sciatica.
5. Although the prognosis is largely determined by the preoperative severity of neurological deficits, early surgery improves the chance of significant recovery so patients with CES require urgent surgical intervention.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
1Emeritus Professor, University of Toronto, Toronto, ON. 2Department of Family and Community Medicine, Baycrest Health Sciences, University of Toronto, Toronto, ON.
Abstract: Urinary tract infections (UTIs) are common in older adults, with prevalence increasing with each decade above sixty-five. UTIs in older adults can be multi-factorial in terms of etiology, risk factors, symptoms, and interventions. A history of heart failure and diabetes increases the risk of UTIs in older adults, and these patients should be closely monitored for symptoms of infection. An enlarged prostate and urinary retention can be an all too common scenario leading to UTIs in older men. UTIs can cause acute confusion and disorientation in older people and should be considered as a possible cause of such new onset symptoms. Physicians should be aware of the variety of presentations and implications of determining a UTI in older adults.
Urinary tract infections (UTIs) are common among the North American population, with prevalence increasing in older adults. Those with a history of heart failure and diabetes are at increased risk.
With the introduction of antibiotics before WWII, and then during the ensuing decades, treatments for UTIs moved away from previously used home-grown remedies.
Physicians should be aware of the variety of presentations and implications of determining a UTI in older adults.
The first case study describes an 84-year-old man with acute onset confusion, disorientation, and urinary retention, who was admitted to the hospital and treated with antibiotics and a small dose of an antipsychotic.
UTIs can cause acute or sub-acute confusion and disorientation in older adults and should be considered as a possible cause of such symptoms.
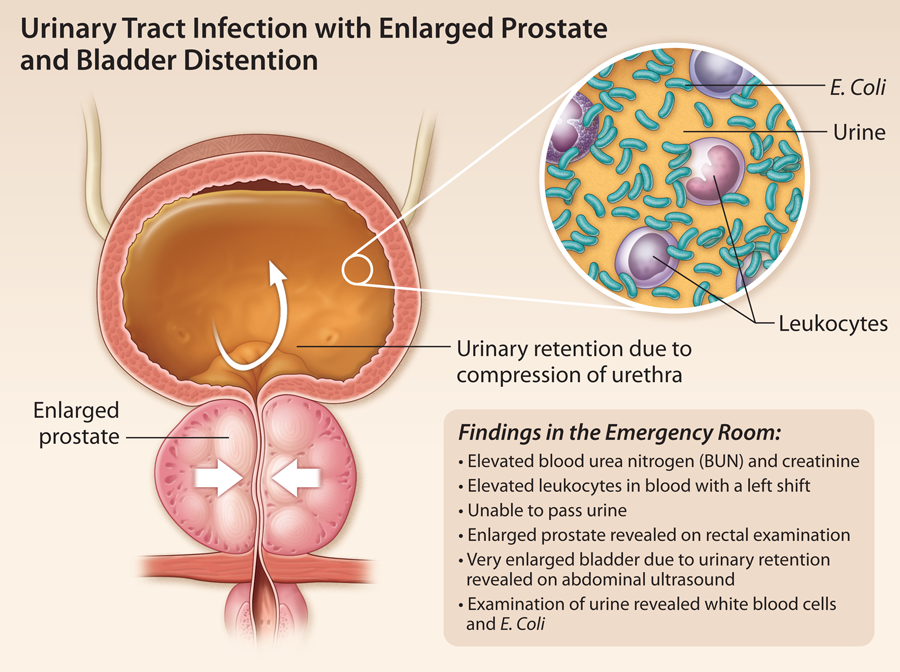
An enlarged prostate and urinary retention is a recognized syndrome of UTIs in older men.
UTIs are a common cause of confusion and disorientation in older adults, and should be considered as a possible cause of these neurological symptoms.
A history of heart failure and diabetes increases the risk of UTIs in older adults, and these patients should be closely monitored for symptoms of infection.
An enlarged prostate and urinary retention can be the underlying cause of UTIs in older adults, and these patients should be evaluated for infection if this constellation of findings exist.
UTIs in older adults can be multi-factorial in terms of etiology, risk factors, symptoms, and interventions, and physicians should be aware of the variety of presentations and implications of determining a UTI in this population.
It is important to use broad-spectrum antibiotics in older adults with UTIs, especially if they are antibiotic-naive patients.
Older adults with UTIs are at risk of harm if they try to remove their catheter or IV; it is important to use soft restraints as needed to ensure patient safety.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Michael J. Borrie, BSc, MB, ChB, FRCPC, Chair, Division of Geriatric Medicine, University of Western Ontario, London, ON.
Acute urinary retention (AUR) occurs predominantly in men and the incidence increases with age. The most common cause of urinary retention is benign prostatic hypertrophy (BPH). For men in their 40s who have no or mild obstructive symptoms (American Urologic Association Symptom Score 7 or less), the incidence of acute urinary retention is 2.6/1000 person years and 3.0/1000 person years in people with moderate to severe symptoms. In contrast, men in their 70's with mild to moderate symptoms have an incidence of AUR of 9.3/1000 person years and this rises to 34.7/1000 person years in those with moderate to severe symptoms.1 Over five years, the risk of AUR for men in their 70s is 10% and for men in their 80s it is almost 30%.1 These findings are based on a cohort of over 2,000 men 40-79, followed over four years and is one of the few longitudinal epidemiologic studies in the area.
Definition Acute urinary retention has been defined as painful inability to void with a urine volume on catheterization of less than 800 ml.2,3 Chronic retention has been defined as the presence of the post-void residual urine volume greater than 500 mls (estimated on bladder ultrasound scan) with or without upper tract dilatation on ultrasound and/or uremia occurring in a patient who is still able to void spontaneously.