is a Family Physician practising Sport and Exercise Medicine at the Toronto Rehabilitation Institute, University Health Network. She is appointed at the University of Toronto, Department of Family and Community Medicine as an Associate Clinical Professor.
Abstract: Clinicians are often unsure if back pain during pregnancy is due to a musculoskeletal condition, an abnormality with the pregnancy or merely part of the common discomforts associated with gestational changes. Low back pain guidelines do not include pregnant women in their criteria and there have been no randomized clinical trials to determine specific causes of low back pain during pregnancy. This article will provide the clinician with a framework for identifying pregnancy-related back pain using a high yield history and key physical examination techniques to differentiate between mechanical back pain, sacroiliac instability and symphysis pubis separation. Risk factors for low back pain and warning signs for pregnancy complications will be identified. Appropriate management strategies will be provided for the management of pregnancy-related low back pain.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
1. Probable Risk Factors for Low Back pain during pregnancy include:
• Pre-pregnancy and past pregnancy low back pain
• Low Back and Pelvic Trauma
• Poor general physical condition
• Joint Hypermobility
• Increase body weight
2. Pregnancy related low back or pelvic pain is defined as intermittent or constant pain in the lumbar, buttock, pelvis, groin and/or upper thigh area lasting for more than one week.
3. Exercise, education and postural advice are the mainstays of treatment and can be enhanced by short term therapy with a rehabilitation professional.
1. Patients who have low back pain, in any trimester, associated with vaginal bleeding, uterine contractions, fever or hematuria should be immediately referred for obstetrical consultation.
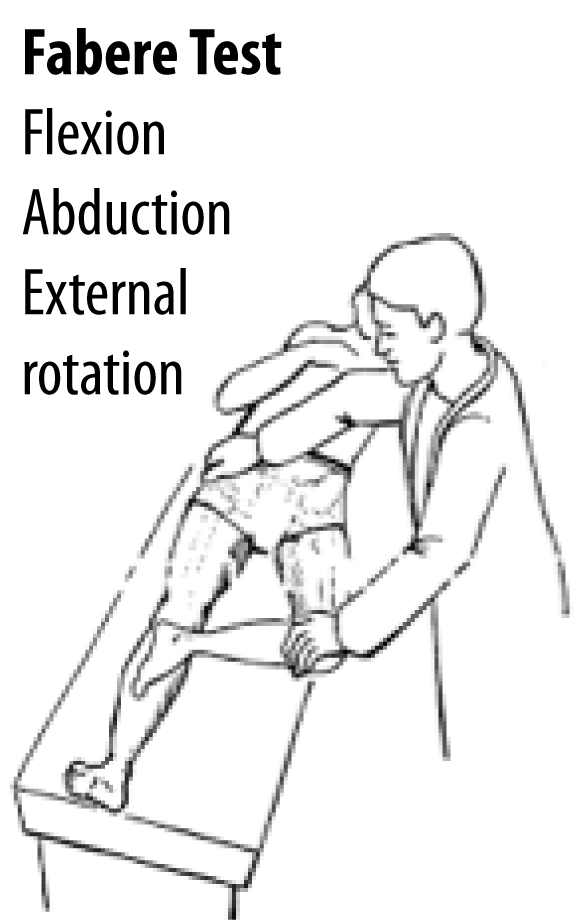
2. The three most common causes of low back pain in pregnancy are mechanical low back strain, sacroiliac instability and symphysis pubis separation; they often occur together.1,2
3. Patient with Symphysis Pubis Dysfunction complain of significant pain during most of these activities:
• Walking
• Climbing Stairs
• Turning in Bed
• Standing on one Leg
• Rising from a Chair
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
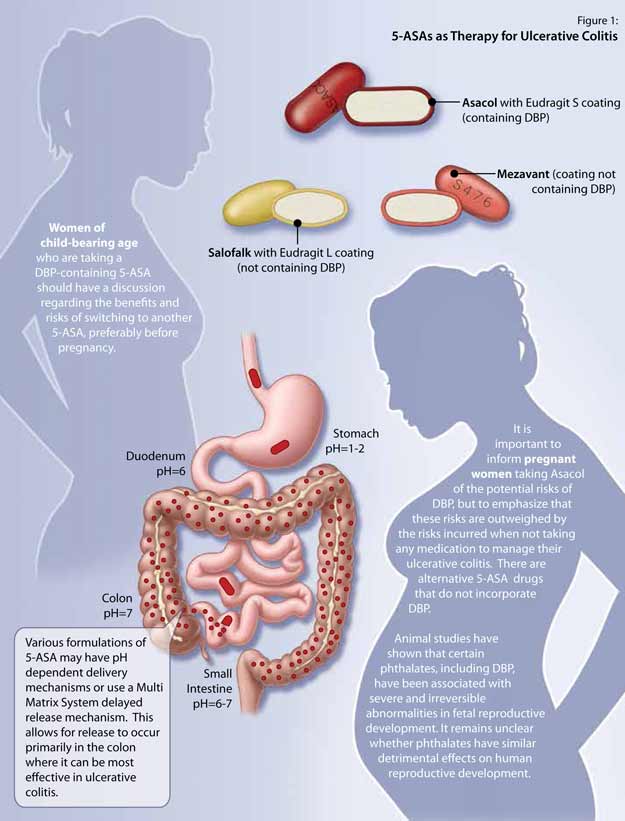
Abstract: 5-Aminosalicylates (5-ASAs) are considered first-line therapy for mild to moderate ulcerative colitis because of their proven effectiveness and safety profile, even in pregnancy. One formulation, however, contains dibutyl phthalate (DBP) in its coating. Though DBP may cause disruptions in utero reproductive development and other congenital abnormalities in rodents, it is unclear whether it leads to physiologically significant fetal abnormalities in humans. The US Food and Drug Administration has changed its classification for DBP-containing 5-ASAs from pregnancy category B to pregnancy category C to reflect a greater degree of uncertainty regarding its effect in humans. For pregnant women with ulcerative colitis, the most important message is to take their inflammatory bowel disease (IBD) medications to prevent disease relapse, which may have the most adverse effects on pregnancy. Physicians should, however, discuss with young women who are taking 5-ASA with DBP the benefits and risks of switching to another formulation of 5-ASA without the DBP compound.
5-Aminosalicylates (5-ASAs) are effective for the treatment of mild to moderate ulcerative colitis and are generally regarded as safe to use, even during pregnancy.
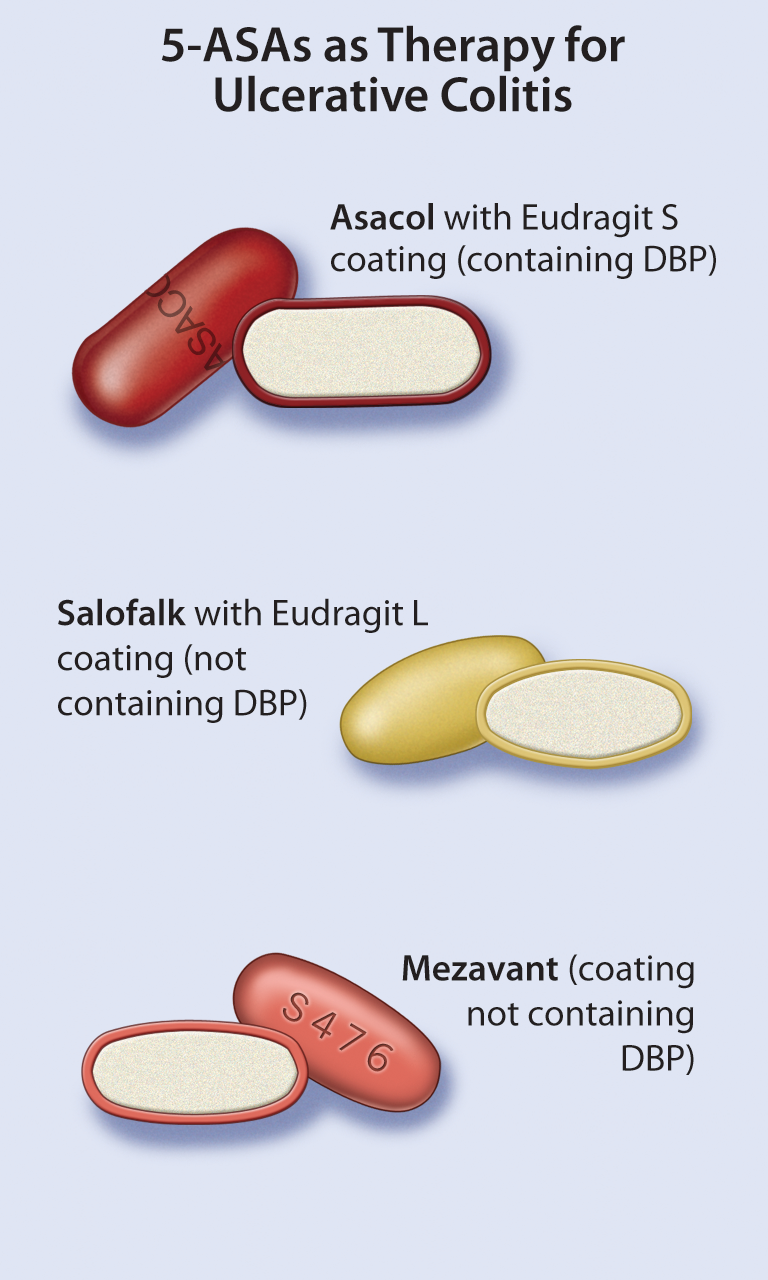
Dibutyl phthalate (DBP) is found in the coating of certain formulations of 5-ASA, and in rodents has been shown to be associated with developmental and congenital abnormalities.
Though phthalates have been shown to be associated with some indicators of reduced masculinization among male fetuses, there is insufficient evidence to prove that it leads to significant harmful effects.
There are several formulations of 5-ASA that do not contain DBP.
Asacol, which contains DBP, is categorized as a pregnancy category C drug, while most other 5-ASAs are in pregnancy category B.
It should be emphasized to pregnant women that taking medications for their inflammatory bowel disease is important because the disease has a strong impact on, not just their health, but the health of their fetus too.
Women of child-bearing age who are taking a DBP-containing 5-ASA should have a discussion regarding the benefits and risks of switching to another 5-ASA, preferably before pregnancy.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Les phtalates dans les 5-AAS : Orienter le choix thérapeutique et minimiser les risques
Teaser:
Geoffrey C. Nguyen, M.D., Ph. D., est professeur de médecine adjoint au Centre for Inflammatory Bowel Disease du Mount Sinai Hospital, Université de Toronto, Toronto (Ontario).
Résumé
Les 5-aminosalicylates (5-AAS) représentent le traitement de première intention pour les patients atteints de colite ulcéreuse (CU) légère à modérée, en raison de leur efficacité prouvée et de leur profil d'innocuité, même pour les femmes enceintes. Cependant, une préparation de 5-AAS possède un revêtement contenant du phtalate de dibutyle (DBP). Bien que, chez les rongeurs, le DBP puisse entraîner des troubles du développement reproducteur et d'autres anomalies congénitales in utero, on ne sait pas si le DBP provoque des anomalies foetales importantes sur le plan physiologique chez les humains. La Federal Drug Administration a modifié la classification des 5-AAS contenant du DBP en les faisant passer de la classe B à la classe C durant la grossesse, afin de refléter le degré plus grand d'incertitude concernant l'effet du DBP chez les humains. Le message le plus important destiné aux femmes enceintes atteintes de CU consiste à prendre les médicaments contre la CU afin d'empêcher une rechute de la maladie, qui pourrait entraîner le plus d'effets indésirables sur la grossesse. Cependant, les médecins doivent discuter avec les jeunes femmes prenant des 5-AAS contenant du DBP des bienfaits et des risques de prendre une autre préparation de 5-AAS sans DBP. Mots clés : phtalates, 5-aminosalicylate, colite ulcéreuse, phtalate de dibutyle, grossesse.