Entreprendre une carrière universitaire : atelier interactif
Conférencier : Kenneth Rockwood, M.D., FRCPC, FRCP, service de gériatrie, Université Dalhousie, Halifax (Nouvelle-Écosse).
En s’adressant à son auditoire, comme clinicien et universitaire, le Dr Kenneth Rockwood a suggéré que la meilleure paraphrase pour décrire la recherche était tout effort, déployé au sein de la médecine universitaire, visant à « améliorer les soins aux patients ».
L’engagement en médecine et en recherche universitaire
Le Dr Rockwood s’est attaché à brosser un tableau de l’engagement professionnel requis en médecine universitaire. Il a prévenu les aspirants universitaires à quel point ils devront consacrer du temps et de l’énergie à leurs activités universitaires, en plus de leur travail clinique. Cependant, les possibilités sont considérables pour améliorer les soins aux patients, et la médecine gériatrique est une spécialité en demande croissante. Après avoir longtemps été le parent pauvre des spécialités médicales, cette discipline voit ses niveaux de rémunération s’harmoniser de plus en plus avec ceux des autres spécialités.
Le Dr Rockwood a rappelé à son auditoire qu’il existe au sein de la communauté universitaire des filières de recherche et d’enseignement, ainsi que des débouchés pour ceux que le travail administratif intéresse. À ceux qui désirent enseigner, il a suggéré que la formation en gériatrie doit continuer à se traduire par une cohérence du corpus des enseignements, et qu’ils doivent tenter de clarifier les principes directeurs qui sous-tendent les savoirs transmis.
Ce qui distingue la gériatrie : l’approche comparative
Pour illustrer son propos, le Dr Rockwood a discuté de la compétence essentielle au cœur de la spécialité. Il a décrit les géria- tres comme devant être des « maîtres de la complexité ». En pratique, cela se traduit par le fait de devoir penser à plusieurs points simultanément. Selon lui, la gériatrie se distingue non seulement par son étendue et sa complexité (embrassant des facteurs tels que l’évolution fonctionnelle du patient, sa qualité de vie future, les résultats de l’examen psychiatrique, la médecine préventive, etc.), mais aussi par un domaine d’action tout à fait unique à cette spécialité.
La médecine gériatrique est avant tout une sous-spécialité de la médecine interne portant sur des personnes âgées fragiles ayant des problèmes complexes, a déclaré le Dr Rockwood. Les gériatres se distinguent des internistes par le fait qu’ils possèdent une vue d’ensemble de la complexité du tableau de santé du patient. À l’opposé, les autres spécialités ont tendance à isoler les problèmes et à les aborder séparément. L’évaluation gériatrique globale, qui recouvre la complexité due à la fragilité, est la marque de la médecine gériatrique.
Cela pose des défis particuliers et apporte des gratifications uniques, a expliqué le Dr Rockwood. En médecine universitaire, les gériatres doivent s’efforcer de transformer les esprits et les comportements, c’est-à-dire permettre à ceux avec qui ils collaborent de saisir la nature des problèmes. De plus, le caractère très glo- bal de la pratique gériatrique sollicite un travail d’équipe multidisciplinaire. Il est parfois difficile d’atteindre l’objectif final, à savoir prodiguer des soins meilleurs, en raison des conflits entre les disciplines et des problèmes de coordination des savoirs de multiples professionnels.
Transmission des savoirs en gériatrie
Le Dr Rockwood a conseillé aux aspirants à une carrière universitaire de ne pas se contenter d’enseigner des sujets pour lesquels ils ont une passion, mais de transmettre également des enseignements et des principes cohérents qui soient à même de transformer les pratiques. C’est le travail d’un passeur de connaissances : transmettre des concepts de façon à ce qu’ils soient utiles à d’autres. Les gériatres qui enseignent et font de la recherche doivent non seulement proposer un ensemble cohérent de connaissances, mais aussi offrir une formation sur les outils cliniques correspondant aux réalités opératoires de la pratique. Il a également mis l’accent sur le fait que l’enseignement doit être réactif et pouvoir s’adapter à l’auditoire.
Le Dr Rockwood a fait remarquer que les gériatres ne sont pas les seuls professionnels de la santé œuvrant dans des situations complexes porteuses de conséquences graves. Par exemple, l’industrie aéronautique développe des procédures et des outils analytiques utiles à la prise de décisions de vie ou de mort en situations complexes. La gériatrie pourrait tirer des connaissances de certains des modes de pensée, d’analyse et d’action adoptés par cette industrie.
En ce qui concerne le développement et l’utilisation du concept de fragilité et des échelles de fragilité en évolution, il a insisté pour que non seulement les cliniciens tiennent compte de la complexité du travail avec des personnes âgées fragiles, mais qu’ils améliorent également leur capacité à discerner les tableaux cliniques. Le Dr Rockwood a fait remarquer à quel point on se sert de signes cliniques non formels pour corroborer une aggravation de la fragilité, et il a demandé aux personnes de l’assistance d’offrir leurs propres indices déductifs (p. ex. : l’incapacité des patients à changer de points de pression). Il a recommandé à ses auditeurs de prêter attention aux difficultés associées au tableau clinique ty-pique ou atypique des patients âgés, faisant remarquer que la gériatrie devait mieux s’intéresser aux plaintes des patients qui ne se sentent pas bien. L’enseignement en gériatrie doit œuvrer à promouvoir les compétences des praticiens en matière de compréhension des patients, a-t-il suggéré.
Acquérir une formation avancée en gériatrie
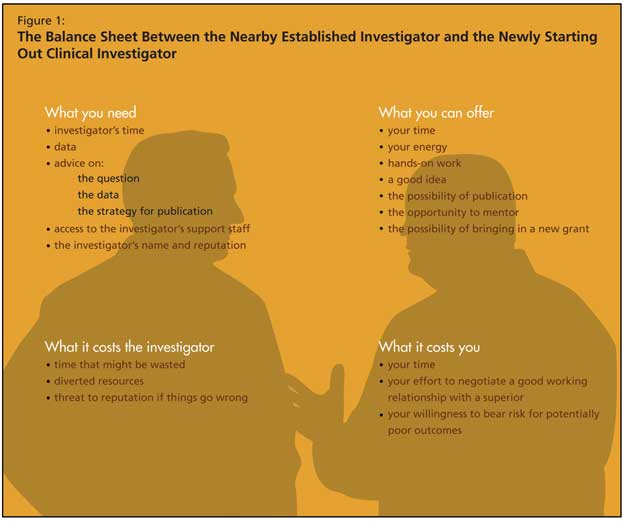
Le Dr Rockwood a offert des conseils concrets pour acquérir une formation avancée en gériatrie. Il a vivement préconisé de choisir un mentor, et a offert des conseils pour établir et approfondir ce type de relation (se familiariser avec le travail du mentor, offrir une assistance de recherche). L’avantage pour l’étudiant? Non seulement il approfondit ses connaissances, mais il accède également aux données et au nom du mentor et à sa collaboration pour des publications. En échange, l’étudiant offre son temps, son énergie, son enthousiasme et ses idées, et représente une promesse de prolonger le travail du mentor (Figure 1). Le Dr Rockwood a suggéré aux aspirants universitaires et aux chercheurs de ne pas trop limiter leurs options avec des travaux de recherche restreints à une seule technologie ou technique thérapeutique, et de prendre soin à ce que leur travail contribue à un ensemble de données cliniques et de recherche se consolidant quotidiennement de façon incrémentale.

Au cours du forum de discussion, le Dr Rockwood a répété que la recherche devait incarner les valeurs personnelles du professionnel de la santé. Il a noté que les médecins non universitaires peuvent travailler en association avec des chercheurs et des universitaires. Il a fait observer que de telles relations de travail sont généralement stimulées par une collaboration avec des universitaires, souvent ouverts à ce type d’engagement. Il a également parlé du travail avec des représentants de l’industrie pharmaceutique, en insistant pour que toute personne engagée dans ce type de travail se souvienne qu’il s’agit d’une proposition d’affaires manifeste de la part de l’industrie. Des renseignements de grande valeur peuvent émerger d’un travail soutenu par l’industrie, a-t-il déclaré. De telles participations représentent souvent des occasions de réseautage avec d’autres médecins ou des groupes avec lesquels un clinicien n’entre habituellement pas en contact.
Selon le Dr Rockwood, les apprentis envisageant d’intégrer le monde universitaire ont surtout besoin de temps, d’argent et de soutien. Le temps devant être consacré aux recherches cliniques est la plus grande exigence de la recherche clinique. C’est ici que l’apprenti établit sa bonne foi, en même temps qu’il développe des relations professionnelles essentielles. En outre, l’aspirant chercheur a besoin de fonds pour acquérir et rémunérer un bon assistant de recherche, ainsi que des subventions de recherche. Finalement, le travail requiert le soutien des autres : à savoir, l’accès à des investigateurs confirmés pouvant se révéler des alliés.