1,2University of California, Davis, Department of Urology, Sacramento, CA, 3Associate Professor, University of California, Davis, Department of Urology and Division of Pediatric Urology, Sacramento, CA.
Abstract: Disorders of sex development (DSD) is an umbrella term for congenital conditions in which anatomic, gonadal, or chromosomal sex is atypical. DSD is found in 7.5% of all births defects and 1 in 5,000 babies born worldwide have significant ambiguous genitalia. Best practices involve multidisciplinary teams, informed consent and shared decision-making with the patient and family. As a group, DSD patients are rare and therefore clinically challenging. Primary care providers, family medicine physicians, and pediatricians are the foundation for patients' medical care and therefore play a key role in the initial diagnosis, guidance, coordination of care, and long-term management.
Key Words:Disorders of sex development, intersex, gender identity, sex differentiation, ambiguous genitalia.
Members of the College of Family
Physicians of Canada may claim MAINPRO-M2 Credits for this
unaccredited educational program.
You can take quizzes without subscribing; however,
your results will not be stored. Subscribers will have
access to their quiz results for future reference.
The most common causes of DSD are congenital adrenal hyperplasia (CAH) and mixed gonadal dysgenesis, constituting approximately half of all DSD cases discovered in newborns.
Initial evaluation of DSD should include a thorough history, physical exam that includes assessment of genital anatomy, evaluation of sex chromosomes using karyotype and fluorescence in situ hybridization, and assessment of internal organs by abdominopelvic ultrasonography.
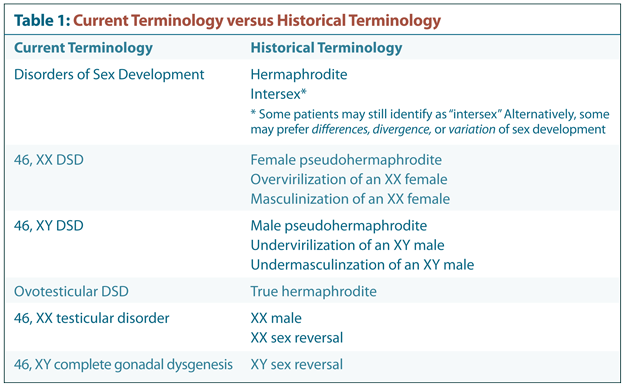
The three classifications within DSD are 46, XX DSD (disorders of gonadal or ovarian development and androgen excess), 46, XY DSD (disorders of gonadal or testicular development and impaired androgen synthesis or action), and chromosomal DSD (numeric sex chromosome anomalies).
Overlooked DSD diagnosis can have the fatal consequence of adrenal crisis due to CAH; phenotypic males with CAH do not present with ambiguous genitalia and therefore adrenal crisis may go undetected at birth.
Physical exam findings that should prompt a DSD workup in neonates include bilateral non-palpable testes, hypospadias in combination with a unilateral undescended testis or non-palpable testes, clitoral hypertrophy, foreshortened vulva with a single urogenital tract opening, and an inguinal hernia with a palpable gonad in a phenotypic female infant.
Initiating the connection to other patients or families and recommending support groups can alleviate isolation, normalize a DSD diagnosis, and encourage positive adaptation.
To have access to full article that these tools
were developed for, please subscribe. The cost
to subscribe is $80 USD per year and you
will gain full access to all the premium content on
www.healthplexus.net, an educational portal, that hosts
1000s of clinical reviews, case studies, educational
visual aids and more as well as within the
mobile app.